
GERD After Sleeve Gastrectomy
Gastric reflux after sleeve is sometimes seen and does not necessarily indicate a complication or abnormal anatomy. Usually it is treated with proton pump inhibitors and will fade over a period of 3-6 months. If GERD is persistent and difficult to control, an upper GI should be done to rule out obstruction. If any obstruction, twist, or kink of the sleeve is noted on upper GI, this needs to be addressed with an upper endoscopy.
Labwork After Sleeve
Typically at post-op month 6 and 12, then yearly thereafter. To see what labs need to be ordered click here.
Marginal Ulcer After Gastric Bypass
A marginal ulcer is an ulcer that occurs at the junction of the gastric pouch with the small intestine. The most common causes of marginal ulcers are smoking and NSAID use. Symptoms typically include epigastric pain and can mimic gallbladder issues. Marginal ulcers are diagnosed with an upper endoscopy. They are usually treated conservatively with smoking and NSAID cessation, PPI’s (omeprazole, etc), and Carafate.
Internal Hernia After Gastric Bypass
An internal hernia occurs when small intestine herniates up into a new opening in the mesentery of the small intestine that gets created during a gastric bypass. Symptoms are abdominal pain, vomiting, and bloating. This can be a life threatening emergency in extreme cases and needs to be corrected immediately with surgery. Diagnosis is usually made by CT scan, however sometimes a scan can miss this problem and exploratory surgery needs to be done to definitively rule it out.
Vitamin Supplements After Gastric Bypass
Patients who undergo gastric bypass require life-long vitamin supplementation. To see what vitamins are recommended click here.
Labwork After Gastric Bypass
Labs are typically checked 6 months after gastric bypass, then as-needed afterwards. To see what labs need to be ordered click here.
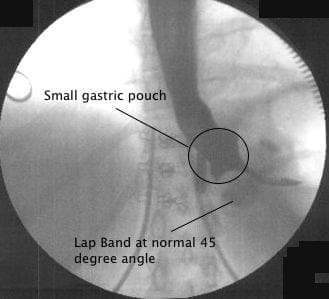
Normal Gastric Band vs. Slipped Gastric Band
In the fluoroscopic pictures below you can see an example of a normal Lap Band, where the band itself is at a 45 degree (3 o’clock to 8 o’clock) angle and there is a small pouch above it, and a slipped band. With the slip the band is at a 10 o’clock to 3 o’clock position and there is a very large pouch above the band.
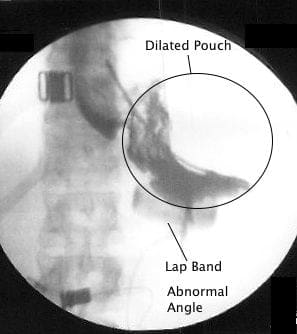
When a band is slipped, the patient will typically have vomiting and GERD issues. The typical treatment is a complete unfill of the band. In some cases the band will go back into position after a few weeks. Sometimes, surgical intervention is required to reposition or remove a slipped band.
GERD After Gastric Band
Gastric reflux is not typical after a Lap Band. New onset GERD in a band patient usually means:
- the band is too tight and needs some saline removed
- the band has slipped
- the gastric pouch above the band is dilated, and acid is pooling there
These patients need to see a band surgeon, not a gastroenterologist!
If you have a patient in this scenario who needs to see us, click here to refer.
Nocturnal Regurgitation After Gastric Band
Nocturnal regurgitation also is not typical after a Lap Band. Similar to GERD, this usually means:
- the band is too tight and needs some saline removed
- the band has slipped
- the gastric pouch above the band is dilated, and acid is pooling there
These patients also need to see a band surgeon, not a gastroenterologist!
If you have a patient in this scenario who needs to see us, click here to refer.
Soft Calorie Syndrome After Gastric Band
Often times when Lap Band patients are not losing weight, they come in to get their band tightened. Sometimes they will get too tight and revert to eating soft calories, such as potato chips and ice cream. These soft foods will go through the band easily, but they cannot eat any protein. This usually leads to weight gain, in spite of a tight band. Patients who have this issue need to have some fluid taken out of their band.
Vitamin Supplements After SIPS
Life-long vitamin supplementation is critical after a SIPS or duodenal switch. To see a list of recommended vitamins click here.
Bloodwork After SIPS
Due to the amount of small intestine that gets bypassed, it is critical for SIPS & duodenal switch patients to have bloodwork done every six months. To see a list of labs that need to be ordered, click here.
GERD After Sleeve Gastrectomy
Gastric reflux after sleeve is sometimes seen and does not necessarily indicate a complication or abnormal anatomy. Usually it is treated with proton pump inhibitors and will fade over a period of 3-6 months. If GERD is persistent and difficult to control, an upper GI should be done to rule out obstruction.
Labwork After Sleeve or Gastric Bypass
Typically at post-op month 6 and 12, then yearly thereafter: CBC, comprehensive metabolic profile, lipid profile, serum iron level, TIBC, serum vit D25 level, serum folate level, serum B12 level, serum B6 level, whole blood thiamine level
