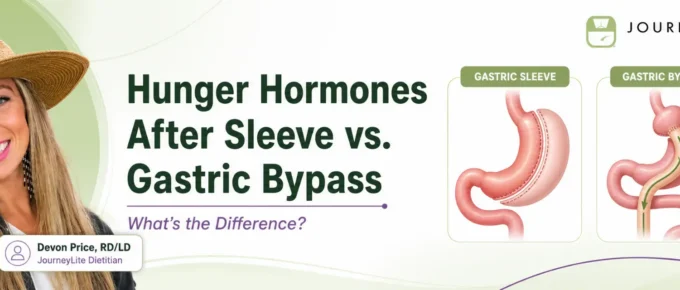
Bariatric nutrition and metabolic health Hunger Hormones After Gastric Sleeve vs. Gastric Bypass: What’s the Difference? Gastric sleeve and Roux-en-Y gastric bypass both …
Continue Reading about Hunger Hormones After Sleeve vs. Gastric Bypass: What’s the Difference? →